
Ever feel a sharp pinch when you reach for a high shelf or struggle to put on a coat? That nagging ache in your shoulder is often more than just "stiffness." For millions of people, it's a sign that the complex machinery of the shoulder joint is struggling. Whether it's a dull throb that keeps you awake at night or a sudden pop during a workout, shoulder pain usually boils down to a few common culprits. The good news? About 80% of these cases get better without surgery, provided you follow a structured plan. If you're dealing with a limited range of motion or a constant ache, understanding exactly what's happening inside your joint is the first step to getting your arm moving again.
Quick Takeaways for Shoulder Recovery
- Most cases are treatable: The vast majority of rotator cuff and bursitis issues respond well to conservative care.
- The "Painful Arc": Pain typically spikes between 60° and 120° when lifting your arm.
- Patience is key: Full recovery usually takes 8 to 12 weeks of consistent exercise.
- Avoid the "Weekend Warrior" trap: Returning to sports too early is a leading cause of relapse.
Understanding the Culprits: Rotator Cuff vs. Bursitis
To fix the pain, you first need to know what's actually irritated. Your shoulder isn't just one joint; it's a sophisticated system of muscles and fluid-filled sacs. At the core, we have the Rotator Cuff is a group of four muscles-the supraspinatus, infraspinatus, teres minor, and subscapularis-that act as a sleeve to stabilize the shoulder joint. When these tendons get inflamed or torn, it's called rotator cuff pathology. This is incredibly common as we age; about 50-60% of people over 80 have some form of cuff damage.
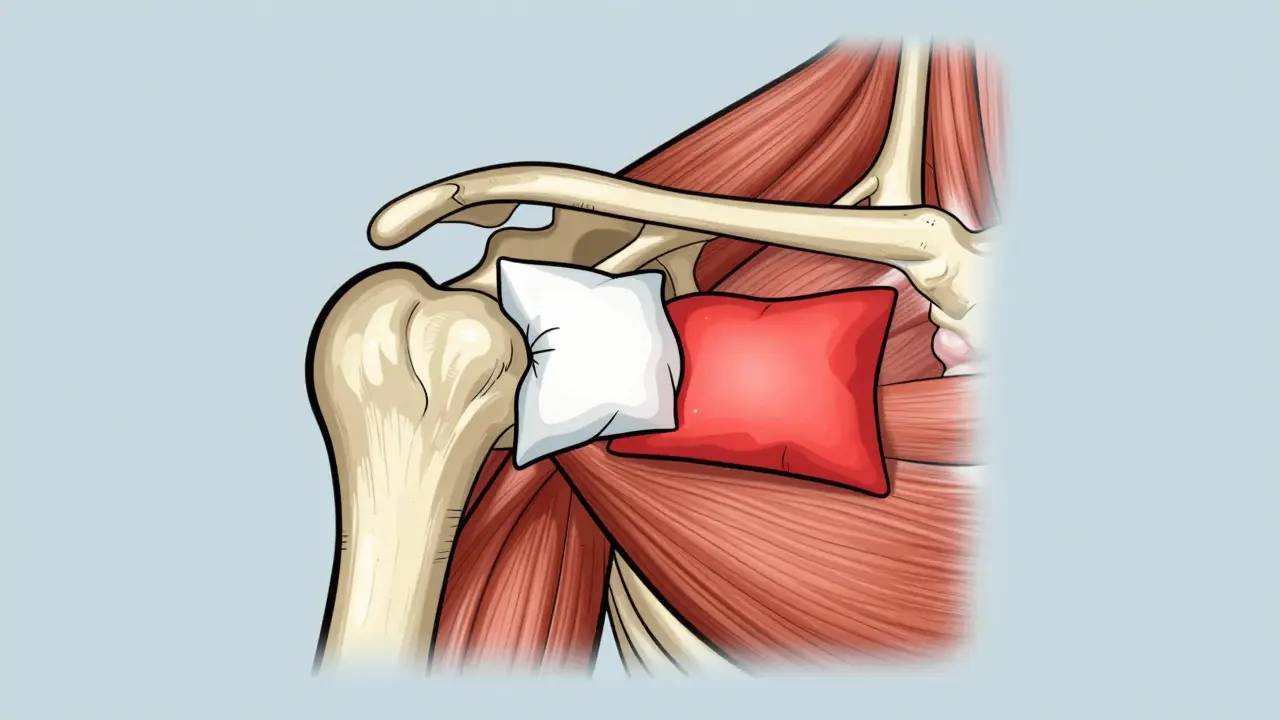
Then there's the bursa. Imagine a small, lubricated pillow sitting between your tendons and the bone. Subacromial Bursitis is the inflammation of the subacromial bursa, a fluid-filled sac that prevents friction between the rotator cuff and the acromion bone. When this "pillow" swells, it takes up too much space. Every time you lift your arm, the swollen bursa gets pinched, creating a cycle of inflammation and pain known as impingement syndrome.
Because they sit so close together, these two often happen at once. You might start with a little tendon inflammation, which irritates the bursa, which then makes the tendon rub even more. It's a frustrating loop, but both respond to similar shoulder rehabilitation strategies.
How to Spot the Warning Signs
Not all shoulder pain is the same. If you're trying to figure out what's going on, look for these specific patterns. The "painful arc" is a classic sign: you feel fine at the start of a lift, but as your arm hits a 60° to 120° angle, the pain spikes, then eases up again as you reach the top.
Night pain is another huge red flag. Many people find it impossible to sleep on their affected side, describing a deep, poorly localized ache. If you're a construction worker or an athlete in a throwing sport (like tennis or baseball), you're at a much higher risk. In fact, construction workers see a 32% higher incidence of these injuries due to repetitive overhead reaching. If your pain is accompanied by a sudden loss of strength-like you can't hold a gallon of milk out in front of you-you might be dealing with a full-thickness tear rather than simple inflammation.
The Roadmap to Recovery: Step-by-Step Rehab
You don't need to jump straight to surgery. Most specialists follow a conservative-first approach. The goal is to calm the inflammation down first, then gradually build strength so the joint doesn't keep pinching.
Phase 1: The Calm Down (Weeks 1-4)
Initially, the goal is "relative rest." This doesn't mean your arm stays in a sling forever, but you should avoid any overhead reaching. Use ice for 15-20 minutes several times a day to bring down the swelling. Over-the-counter NSAIDs, like ibuprofen, are often used here to break the inflammation cycle. If the pain is too intense to even start moving, a corticosteroid injection might be used. While these are great for a quick reset, experts warn against getting more than 2-3 a year, as too many can actually weaken the tendons.
Phase 2: Gentle Motion (Weeks 2-6)
Once the sharp pain subsides, you start with Pendulum Exercises is a low-impact rehabilitation technique where the arm hangs loosely and swings in small circles to maintain joint mobility without stressing the muscles. These are usually started within the first few days. From there, you move into active-assisted range of motion, where you use your "good" arm or a stick to help guide the injured arm through its movements.
Phase 3: Strengthening (Weeks 6-12)
This is where the real work happens. You'll introduce resistance bands (like TheraBands) to strengthen the cuff. The secret weapon here is scapular stabilization. Most people focus only on the arm, but squeezing your shoulder blades together-scapular retraction-is crucial. Patients who prioritize these "blade" exercises often see pain resolve 30% faster than those who only do arm curls.
| Approach | Estimated Cost | Recovery Time | Success Rate | Main Risk |
|---|---|---|---|---|
| Physical Therapy | $1,500 - $3,000 | 3 - 6 Months | ~80% | Slow progress/Relapse |
| Steroid Injections | $200 - $600 | Immediate/Short-term | 65 - 75% | Tendon weakening |
| Surgery (Arthroscopy) | $15,000 - $20,000 | 4 - 6 Months | Variable | Surgical complications |
When Physical Therapy Isn't Enough
If you've spent three months doing your home exercises and you're still waking up in pain, it might be time to discuss surgical options. The most common procedure is Arthroscopic Subacromial Decompression is a minimally invasive surgery where a surgeon removes inflamed bursa tissue and shaves the acromion bone to create more space for the tendons.
This is generally reserved for people with bone spurs that physically block the tendon or for those with full-thickness tears. For a 60-year-old with a complete tear, the healing rate with just exercise is only about 40%, compared to 75% for a partial tear. In these cases, surgery isn't just an option; it's often the only way to regain full strength. However, for isolated bursitis without a tear, surgery often shows very little benefit over a dedicated physical therapy program.

Pro Tips for Better Results
Recovery isn't a straight line. You'll likely encounter the "pain paradox": the feeling that you have to push through some discomfort to get better, but not so much that you re-injure yourself. A good rule of thumb is the 0-10 pain scale. If your exercise keeps you below a level 5, you're generally safe. If you hit a 7 or 8, back off.
To stay on track, use technology. People who use smartphone apps for exercise reminders are significantly more likely to finish their rehab and recover 27% faster. Also, don't stop the moment you feel "better." The "weekend warrior" effect happens when someone feels 90% recovered, goes out and plays a full game of pickleball or tennis, and immediately triggers a relapse. Stick to the protocol until your therapist clears you for full activity.
How long does it take for shoulder bursitis to heal?
Most people see significant improvement within 8 to 12 weeks. This timeline includes an initial phase of reducing inflammation (2-4 weeks) followed by a progressive strengthening program. Consistency with home exercises is the biggest factor in how quickly you recover.
Can I use ice or heat for shoulder pain?
In the acute phase-when the pain is sharp and the area may feel warm-ice is your best friend. Apply it for 15-20 minutes several times a day to reduce swelling. Once the inflammation has settled and you're starting strengthening exercises, gentle heat can help loosen the muscles and improve blood flow before your workout.
Are steroid injections safe for the rotator cuff?
They are effective for short-term pain relief, but they come with a trade-off. Frequent injections (more than 3 per year) can lead to tendon weakening and increase the risk of a rupture by about 8%. They should be used as a tool to make physical therapy possible, not as a permanent cure.
What is the difference between a rotator cuff strain and a tear?
A strain (or tendinitis) is an inflammation or irritation of the tendon. A tear is a physical rip in the muscle or tendon. Partial tears can often be managed with rehab, while full-thickness tears-where the tendon is completely detached from the bone-often require surgery to restore full function, especially in older adults.
Should I completely immobilize my arm if it hurts?
Generally, no. While strict rest is needed for the first few days of a severe acute injury, total immobilization for too long can lead to "frozen shoulder" (adhesive capsulitis). Most guidelines suggest starting gentle range-of-motion exercises, like pendulums, within 48 to 72 hours to keep the joint lubricated.
Next Steps for Your Recovery
Depending on where you are in your journey, your next move will differ:
- If you're in the acute phase: Focus on the "Calm Down" phase. Ice, activity modification, and a visit to a doctor to confirm the diagnosis.
- If you've been in pain for weeks: Book an appointment with a physical therapist. Ask specifically about scapular stabilization and a home exercise plan with videos.
- If you've tried rehab for 3+ months without progress: Request a T2-weighted MRI or an ultrasound. This will show if there is a structural tear that requires surgical intervention.
Vivek Hattangadi
The part about scapular stabilization is honestly a game changer for anyone dealing with this. I've seen so many people just focus on the arm and wonder why they aren't getting better, but getting those shoulder blades moving correctly is where the magic happens. Just keep at it, everyone! Consistency with those TheraBands really pays off in the long run.