
Opioid Dose Calculator for Liver Disease
Recommended dose: 0 mg
Dosing interval: 0 hours
Based on clinical guidelines for opioid use in liver disease. Always consult with your healthcare provider.
Note: These are general guidelines. Individual patient factors may require further adjustments.
When someone has liver disease, taking opioids isn’t just a matter of adjusting the dose-it’s a completely different game. The liver doesn’t just filter toxins; it breaks down pain medications like morphine, oxycodone, and others. When it’s damaged, those drugs don’t clear the way they should. Instead, they build up. And that buildup can turn a helpful pain reliever into a dangerous threat.
How the Liver Normally Handles Opioids
The liver uses two main systems to process opioids: the cytochrome P450 enzymes and glucuronidation. These are the body’s way of turning drugs into forms that can be flushed out through urine or bile. For example, morphine gets turned into two metabolites: morphine-6-glucuronide (M6G), which helps with pain relief, and morphine-3-glucuronide (M3G), which can cause seizures and confusion. Normally, the liver clears these quickly. But in liver disease, this system slows down.
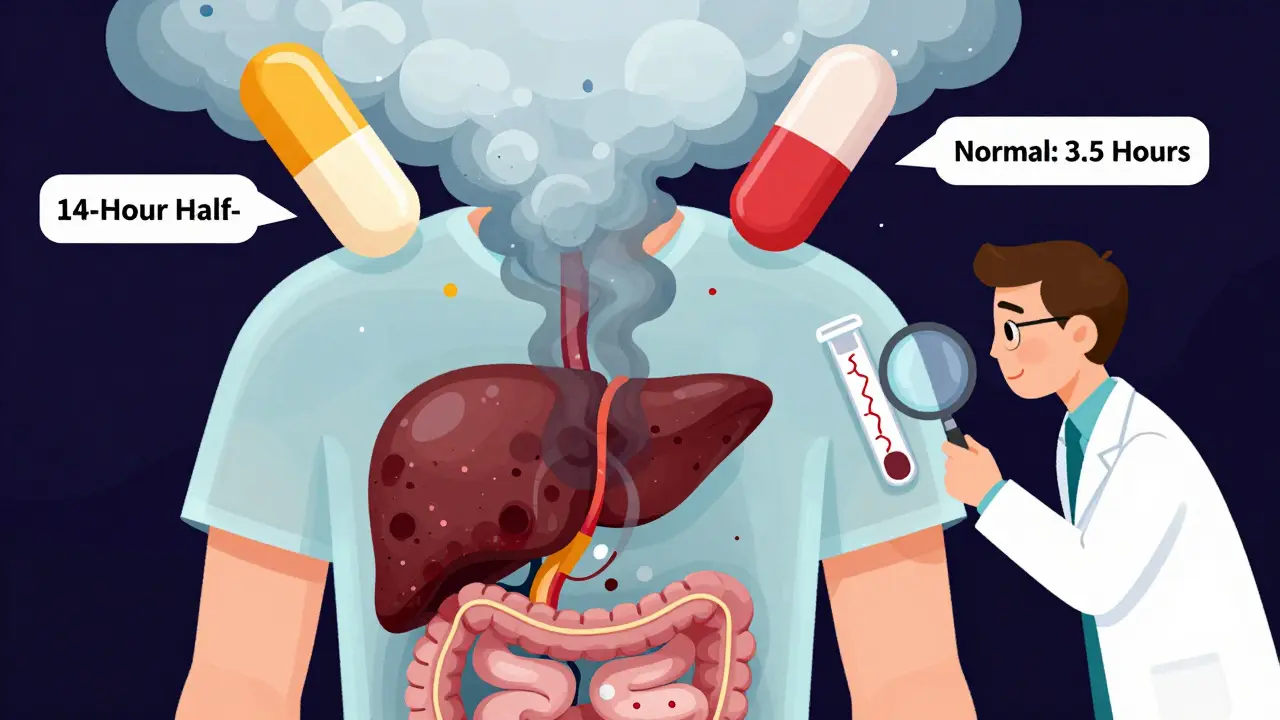
Oxycodone is broken down by CYP3A4 and CYP2D6 enzymes. In healthy people, it leaves the body in about 3.5 hours. In someone with advanced liver failure, that time jumps to an average of 14 hours-and can stretch as long as 24 hours. That means the drug stays in the bloodstream much longer, increasing the chance of overdose even if the dose hasn’t changed.
Why Liver Disease Changes Everything
Liver disease isn’t one thing. It comes in many forms: alcohol-related, fatty liver, hepatitis, cirrhosis. Each one affects drug metabolism differently.
In non-alcoholic fatty liver disease (NAFLD) and diabetes, CYP3A4 activity drops. That means drugs like oxycodone and fentanyl stick around longer. In alcohol-related liver disease, CYP2E1 goes into overdrive. This enzyme can create toxic byproducts when breaking down opioids, adding another layer of risk.
And it’s not just about how fast the liver clears the drug. The liver also produces proteins that bind opioids in the blood. When liver function declines, fewer binding proteins are made. That means more of the drug is free and active in the bloodstream-even at normal doses. This is why people with cirrhosis can feel the effects of a low dose as if it were a high one.
Specific Opioids and Their Risks
Not all opioids are created equal when the liver is damaged.
- Morphine: Its metabolites are the biggest concern. M3G builds up and can cause neurological side effects like tremors, hallucinations, and seizures. In early liver disease, doctors often cut the starting dose by 25%-50%. In advanced failure, they also space doses further apart-sometimes giving the same dose only every 8-12 hours instead of every 4-6.
- Oxycodone: Because its metabolism is so heavily dependent on liver enzymes, the starting dose should be reduced to 30%-50% of the normal amount in severe liver impairment. Even then, patients need close monitoring for drowsiness and breathing problems.
- Methadone: It’s metabolized by several CYP enzymes, so it’s less likely to build up from one single pathway. But there’s no clear dosing guide for liver disease. That makes it risky unless carefully managed by a specialist.
- Fentanyl and Buprenorphine: These are often used in liver disease because they’re given through patches or injections, bypassing the liver’s first-pass metabolism. Still, long-term use in cirrhosis hasn’t been well studied. Their safety is assumed, not proven.
More Than Just Toxicity: Gut Damage and Inflammation
The problem doesn’t stop at metabolism. Long-term opioid use can harm the gut. Opioids slow bowel movement, change gut bacteria, and increase intestinal permeability. This lets toxins from the gut leak into the bloodstream. The liver, already struggling, now has to deal with these extra toxins. This triggers inflammation, which can make liver disease worse.
Studies show this gut-liver connection is real. In people with cirrhosis who take opioids regularly, markers of liver inflammation go up faster than in those who don’t. It’s not just the drug itself-it’s how the drug changes the body’s internal environment.
What Doctors Need to Do
Guidelines are clear: don’t treat liver disease patients the same as healthy ones. But many doctors still do.
Start low. Go slow. Monitor closely. That’s the rule. For morphine, even mild liver impairment means cutting the initial dose. For oxycodone, it’s not just a 50% cut-it’s also doubling the time between doses. Some patients need to switch to non-liver-metabolized painkillers like tramadol (with caution) or non-opioid options like gabapentin or acetaminophen (in very low doses).
Regular blood tests aren’t enough. Doctors need to watch for signs of toxicity: confusion, extreme drowsiness, slow breathing, or unexplained nausea. These aren’t just side effects-they’re warning signs of overdose in someone whose body can’t process the drug.
What’s Still Unknown
There’s a big gap in the science. We don’t have solid dosing rules for most opioids in liver disease. Most guidelines are based on small studies or expert opinion, not large trials.
We don’t know how fentanyl patches behave in patients with severe cirrhosis. We don’t know if buprenorphine is truly safer long-term. We don’t know if certain types of liver disease-like autoimmune hepatitis-react differently than alcoholic cirrhosis.
And we still don’t have a good way to measure how much opioid is too much in someone with liver damage. Blood levels aren’t reliable. Symptoms are the best guide-but they’re often missed until it’s too late.
Bottom Line: A Dangerous Combination
Opioids and liver disease are a dangerous mix. The liver isn’t just a filter-it’s the gatekeeper. When it fails, the gate opens wide. Drugs that are safe for most people become risky, even deadly, for those with liver damage.
There’s no one-size-fits-all solution. Each patient needs individualized care. Dose reductions, longer intervals, careful monitoring, and alternative pain strategies aren’t optional-they’re essential. Ignoring the liver’s role in opioid metabolism isn’t just outdated-it’s dangerous.
Aileen Nasywa Shabira
Oh wow, so the liver's just a lazy bouncer at a club now? 'Sorry, pal, your morphine's got a VIP pass but your liver's closed for renovations.' I'm sure every ER doc is just thrilled to play Russian roulette with dosing.
At least we can all agree that if you're on opioids and your liver looks like a crumpled paper bag, maybe you should've stopped drinking before the 4th beer.
Kendrick Heyward
This is why we need to stop enabling addicts. You can't just give people pain meds like candy because they made bad life choices. The liver doesn't care how 'sick' you feel-you broke your own body. Now we're all paying for it with higher drug costs and ER bills.
God help us when the next generation grows up thinking their body is a vending machine.
lawanna major
It's fascinating how the body is a system of interdependent processes. The liver doesn't just 'process' opioids-it's part of a delicate ecosystem that includes gut flora, immune signaling, and even neurological feedback loops. When one part falters, the whole architecture trembles.
What we're seeing isn't just pharmacokinetics-it's the body's symphony going off-key. And the tragedy isn't that people need pain relief-it's that our medical system still treats organs like interchangeable parts.
Ryan Voeltner
The clinical implications of hepatic impairment on opioid metabolism are profound and demand a paradigm shift in pain management protocols. Standard dosing algorithms fail to account for nonlinear pharmacokinetic changes in cirrhosis.
Individualized titration remains the gold standard. Evidence supports cautious use of transdermal fentanyl and buprenorphine in this population, though long-term data are sparse.
Collaborative care involving hepatology and pain specialists is not optional-it is imperative.
Linda Olsson
Of course they say 'start low, go slow.' That's what they said about OxyContin in '99. Then the pharmaceutical reps showed up with free dinners and 'educational grants.'
Do you really think this is about patient safety? Or is it about keeping the opioid pipeline flowing while doctors get paid per prescription? The liver doesn't lie-but the FDA sure does.
Ayan Khan
In many cultures, pain is seen as part of the human experience, not something to be erased with chemicals. I have seen elders in rural India manage chronic pain with turmeric, yoga, and community support.
Perhaps the real issue is not just liver metabolism-but our over-reliance on pharmaceuticals as the only solution. We forget that healing is not just chemical, but relational.
Emily Hager
This article is a textbook example of medical liberalism gone rogue. The liver is not a 'gatekeeper'-it's a biological organ that functions according to laws of chemistry, not metaphorical poetry.
And yet here we are, anthropomorphizing organs and treating patients like fragile porcelain dolls. The truth? People with liver disease should be advised to avoid opioids entirely-not given a 30% reduction and a pat on the head.
Melissa Starks
I work in a clinic and let me tell you, this is REAL. I had a lady last week on 30mg oxycodone every 6 hours-liver cirrhosis from years of drinking. She was nodding off in the waiting room. We cut her to 10mg every 12 hours and her daughter cried because 'she doesn't feel like herself.'
But here's the thing-she stopped falling. She stopped confusing her meds. She started talking to her grandkids again.
It's not about the 'high.' It's about being present. And sometimes, less is more. I wish more docs understood that.
Lauren Volpi
So let me get this straight-we're gonna tell people with liver damage to 'go slow' on painkillers while the government pushes fentanyl patches like they're candy?
Meanwhile, the same people who wrote this article are probably on their third Xanax and a 6-pack of craft beer. Hypocrites.
Real solution? Stop giving people pain meds. Teach them to suffer. Like our ancestors did. Back in the day, no one had a liver and still walked around like a zombie.
Kal Lambert
Buprenorphine patches are underused in liver disease. Lower risk of respiratory depression. Less reliance on CYP metabolism.
Still need monitoring. But it's the best tool we have right now.
Tramadol’s a no-go-CYP2D6 and serotonin risks. Stick to non-opioids first. Acetaminophen <2g/day. Gabapentin. Physical therapy.
Simple. Safe. Effective.
Melissa Stansbury
I just want to say thank you for writing this. My mom has cirrhosis and they kept giving her morphine like she was 25. She was confused for weeks. We almost lost her.
It’s not just about the drugs. It’s about doctors not listening. I’m so glad someone’s finally saying this out loud.
cara s
I read this article at 3am while nursing my third cup of coffee and wondering why my liver enzymes are up.
Turns out I've been taking ibuprofen for my back pain for 8 years.
And now I'm Googling 'can you get liver damage from ibuprofen?'
Also I think I'm allergic to responsibility.
Anyway. This. This right here. This is why we need more people like you writing this stuff.
And also, I'm switching to acupuncture. Or maybe just yelling at my back until it feels better.
Amadi Kenneth
This is all a lie. The liver doesn't metabolize opioids. It's the government. They put nanobots in the meds to track us. The 'metabolites' are just data packets. The 'dose reduction' is a cover for the CIA shutting down our pain signals so we don't notice the 5G towers in our water.
Also, the FDA is run by Big Pharma puppets who are secretly aliens.
Ask your doctor if your morphine is truly yours-or if it belongs to the deep state.
becca roberts
Oh honey, you just described my ex-husband’s entire life. 'Oh, I'm in pain!' 'Oh, here's a pill.' 'Oh, I'm still in pain!' 'Here's another pill.' 'Oh, I'm confused and can't find my pants!' 'Here's a third pill.'
At least now we know why he kept asking for the remote control to 'turn off the pain.'
Love you, but maybe next time, try a massage?
Andrew Muchmore
The data supports reduced opioid dosing in liver disease. Guidelines exist. Implementation is inconsistent.
Education gaps persist.
Systemic change is needed.
Start now.